Medical groups are sending mixed messages about when to begin routine mammograms and how often to get them, and that disagreement matters for millions of women across the U.S. Experts such as Dr. Laura Esserman at the University of California, San Francisco, and Dr. Carolyn Crandall at UCLA weigh the trade-offs, while public health researcher Robert Smith of the American Cancer Society explains why recommendations diverge. This piece walks through the split guidance, what dense breasts and genetics mean for screening, and how new approaches like risk-based testing and AI may change the rules.
Deciding when to start regular mammograms can feel like navigating a maze because different organizations endorse different ages and intervals. Some panels now say start at 50 and screen every other year, while others recommend beginning in the early 40s with annual or biennial checks. The result is confusion for women and doctors trying to balance catching cancers early against the harm from false alarms and unnecessary procedures.
Part of the problem is the one-size-fits-all nature of many guidelines, which are aimed at women at average risk with no symptoms. “Breast cancer is not one disease,” said Dr. Laura Esserman of the University of California, San Francisco. She argues it makes little sense to treat everyone the same when individual risk varies so widely, and she is running studies to refine screening based on a person’s unique profile.
Breast cancer remains common: more than 320,000 women in the U.S. will likely receive a diagnosis this year, and though death rates have fallen thanks to better treatments, it is still the second-leading cause of cancer death in women. That prevalence makes it hard to define what “average risk” actually means, because many people carry risk factors that tip them away from the average. Age has traditionally been the clearest risk marker, since incidence rises as women get older, but genetics, family history and lifestyle also matter.
Guidelines differ sharply. The American College of Physicians recently recommended that women ages 50 to 74 at average risk get a mammogram every other year, and that those 40 to 49 discuss pros and cons with their doctor before deciding on biennial screening. The U.S. Preventive Services Task Force now suggests starting biennial screening at 40, while the American Cancer Society advises yearly mammograms for ages 45 to 54, allowing women to begin at 40 if they choose. These variations reflect different judgments about how to weigh benefits against harms.
Mammograms can miss cancers and sometimes pick up harmless anomalies that lead to stress, biopsies and other follow-ups. “We’re not saying there’s no benefit” from mammograms in the 40s, cautioned Dr. Carolyn Crandall of the University of California, Los Angeles, who chaired the American College of Physicians report. But she noted that “there’s a narrower balance between the benefits you could get and the harms in 40- to 49-year-olds.” That narrower balance is why panels disagree about recommending routine screening for that decade.
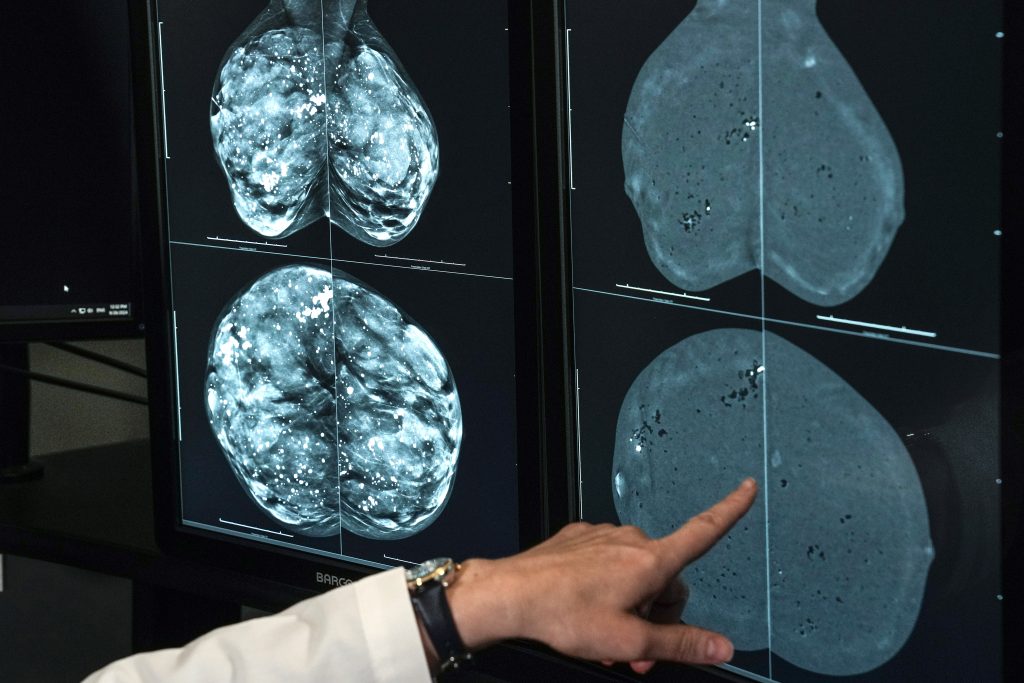
Breast density further complicates screening choices. Nearly half of women over 40 have dense breast tissue, which makes tumors harder to spot on standard mammograms and slightly raises cancer risk. Women now typically receive a density notification after imaging, but experts say it’s still unclear whether adding ultrasound or MRI to routine screening helps most people with dense breasts. Some clinicians do favor 3D mammography, also called digital breast tomosynthesis, as an alternative that can improve detection in certain cases.
Researchers are exploring ways to move beyond age alone, using genetic screens and comprehensive risk models to personalize screening schedules. The WISDOM trial studied nearly 46,000 women and classified participants using age, genetics, lifestyle, health history and breast density to set individualized intervals. Esserman’s team reported in JAMA that risk-based screening performed about as well as standard annual mammograms, and the study revealed that about 30% of women flagged by genetic testing had no known family history of breast cancer.
AI is also entering the picture as a possible tool to extract hidden risk signals from mammogram images and predict a woman’s likelihood of developing breast cancer in the near term. If validated, such tools could point to who needs more frequent checks and who might safely wait longer between images. For now, these approaches are experimental but promising, and they point toward a future where screening is tailored rather than uniform.
Meanwhile, practical steps still matter: talk with your doctor about relatives who have had breast cancer, your overall health, childbearing history and other risk factors that might change your screening plan. Whatever interval or starting age you choose, consistency is important—Robert Smith, the American Cancer Society’s expert on early detection, put it plainly: “Breast screening works best when it’s done regularly.”








